NOT WELCOME ANYWHERE: EXCLUSION AND INACCESSIBILITY OF LEGAL, MEDICAL AND SOCIAL SERVICES FOR PEOPLE WHO TRADE SEX AND USE DRUGS
MOTIVATIONS AND INTENTIONS
PROJECT DAWN COURT: Philadelphia’s Prostitution Diversion Program
EXPERIENCES OF EXCLUSION: (IN)ACCESS TO SOCIAL SERVICES
EXCLUSION FROM SOCIAL AND LEGAL SERVICES
EXPERIENCES OF DISCRIMINATION: NOT WELCOME ANYWHERE
ENCOUNTERS WITH VIOLENT SYSTEMS AND INSTITUTIONS: LAW ENFORCEMENT, PRISONS AND COURTS
MOTIVATIONS AND INTENTIONS
Project SAFE is a harm reduction organization for women and queer individuals in Philadelphia that works at the intersection of drug use, sex work and homelessness. Nearly all of our members have been harmed by law enforcement and the criminal justice system and have sought to reduce that harm through various means, including participating in diversion programs and social services. We have been talking with our members about the role of diversion programs in reducing the harms of arrest and incarceration for years. Our members have expressed mixed views about both their existence and effectiveness. Some members have reported that they have benefitted from the services they received, but many of our members have had difficulty accessing diversion programs and face barriers to completing them in the event that they are admitted. For some, diversion is simply delayed incarceration. Our members have also shared their difficulties in accessing other services including medical and mental health care, legal aid, and social service programs, due to being stigmatized as people who use drugs and engage in sex work. To that end, we decided to design and conduct a community-led survey in order to capture our members’ experiences of accessing and engaging in both diversion programs and social services, since these were the two primary ways that our members sought to reduce the harms they experience in their lives.
This community-based and led project is different from research done by and for institutions, such as universities and government agencies, that can exploit the experiences of sex workers. Our community-led survey is designed and carried out by sex workers, for the benefit of sex workers. In the spirit of “nothing about us, without us” the information that follows is our response to policy issues impacting our communities where our voices are often not heard. Furthermore, our expertise in creating reports like this is a vital part of transforming the way research is done.
DEFINING TERMS
Sex Work – any and all erotic labor involving exchange of services for cash, goods and other needs; this includes, but is not limited to: street-based sex work, escorting, exotic dancing, adult film performance, domination, kink play, webcam performers, and sugar babying. We conceptualize policing of sex work as existing on a continuum of labor and rights violations. The less autonomy one has over their working conditions, the more exposure there is to risk and harm such as violence and health impacts, such as sexually transmitted infections (STIs). In addition, risk levels are dependent on venue; some harms such as arrest and interactions with law enforcement are amplified for workers who do not have access to private working spaces. Street-based sex workers who are doing dates in cars or in alleys are more likely to be arrested or harassed by law enforcement officers.
Labor rights: the recognition that all workers have the right to fair working conditions and pay, and the right to collectively organize to defend workers and work sectors from the influence of employers, owners of businesses and other actors. The right to organize is also described as freedom of association in human rights law.
Human Trafficking: The use of coercion, abuse and/or deceit to force individuals to engage in labor and depriving them of their freedoms over an extended period of time in a systematic and continuous manner. Sexual violence occurs as a form of control across all types and sites of trafficked labor.
Drug Use: any consumption of a substance from injection to drinking of illicit, licit and repurposed pharmaceutical substances or undefined substances. We use the acronym PWUDs for people who use drugs.
Harm Reduction: A philosophy that seeks to ameliorate the harms inherent to any human activity, and the strategies to accomplish that goal. Within the context of drug use they focus on the biological/pharmacological effects of using a substance together with coping with the social and psychological harms inflicted by the systems around each substance.
Medical Trauma: trauma incurred when experiencing stigma and discrimination from staff in medical and mental healthcare settings. Examples include medical providers minimizing or dismissing symptoms and lived experiences of their patients, security guards profiling patients in the ER as people who use drugs and searching them for drugs and drug use equipment, asking unnecessary and intrusive questions, denying services and forcing individuals to comply with unwanted treatments and procedures, etc.
Terms to think critically about:
Survival Sex Work: Much like in other industries, a range of class locations exist in sex work. Some sex workers are able to access upward class mobility while most sex workers find themselves surviving off of their sex work wages or supplementing it with other underground or above ground economic activities. We find these conditions similar to many other laborers in working class condition and hence reject the term survival sex work.
The term survival sex or survival sex work creates a false binary. It presumes a lot about what we can tell about the material conditions of workers and what their survival goals are from both the rates they charge and how they’re presenting themselves in their work personas. For example, one person’s goal may be a steady supply of drugs while another worker’s may be to pay necessities month to month, go to college or buy a car. People in the same class category of sex work, and often charging the same rate, could be housed or unhouse, could be street based workers or working online. Often, sex workers play “class drag”, that is, present to be in a higher class than they actually are in, as an attempt to reduce work place violence experienced as sex workers. Additionally, sex workers of color and trans sex workers always face a different type of violence related to their marginality regardless of how much they are able to charge. Hence, survival sex as a term does not tell us much about the risks a sex worker faces or their working conditions. Indeed, all workers under capitalism are trying to survive state-sanctioned poverty, which comes in many different forms. Yet, we do not have “survival domestic worker” or “survival food industry work” as terms to denote class in concurrent service industries. We find that “survival sex work” often harkens back to stigmas arising from anti-Blackness and poverty mapped on to sex work.
Addict: This term has been medicalized to allude to an individual in the grips of “addiction,” a loosely defined word referring to the compulsive use of any substance or behavior. It lacks person-first language and generalizes people who use drugs to individuals who lack agency or control over their drug use. However, many people who use drugs define themselves as “addicts,” which is arguably rooted in abstinence-based, 12-step philosophies. When referring to others, we use the term people who use drugs [PWUDs] or people who inject drugs [PWIDs].
Prostitute: The term is colloquial and stigmatized in social work and criminal justice. It fails to contextualize sex work as labor and therefore, works to keep a labor practice criminalized. People in the community who may be supportive of sex work but may not know terms may still use prostitution.
Pimp: a term often used in news media to refer to men who recruit, abuse and traffic women. The term is racialized and is often used to refer to Black men and perpetuates stereotypes about them as criminals and misogynists.
Sex Trafficking: In the U.S. legal system, this term refers literally to the trafficking of sex and not to the trafficking of human beings for sexual exploitation (Chapman-Schmidt 2019). Chapman-Schmidt argues that the term, which displaces “both the language and social spaces used by sex workers, constitutes a form of epistemic violence, and that this epistemic violence leads, in turn, to an increase in physical violence against sex workers. This is evident in the passage of laws such as SESTA-FOSTA, which led to the shutdown of important online spaces where sex workers communicated with each other such as the Reddit board r/escort and to the disappearance of online safety tools. After the Trafficking Victims Protection Act was passed in 2000, some states also began targeting sex work clients as “sex traffickers.” States have also used the framing of sex workers as sex trafficking victims to establish diversion programs (i.e. New York) and to justify ongoing arrests and prosecution as a way to help sex workers escape from trafficking (Texas).
Opioid epidemic: We steer clear of this term as opioids in and of themselves are not a crisis. Opioids, in fact, improve the quality of life of individuals every day. The crises associated with opioids include the adulteration of unregulated opioids with fentanyl, benzodiazepene-related drugs, and other psycho- and non-psychoactive substances, which have led to the catastrophic opioid overdose fatality throughout North America. Additionally, the dramatic reduction in opioid prescribing as a means of primary prevention of drug use has led to a pain crisis, meaning that pain being undertreated has led to people in pain relying on the unregulated drug market to access adequate medicine to treat their pain.
Paraphernalia: A term used by the criminal justice system for charges related to the possession of drug administration equipment (e.g. injection and smoking equipment).
WHY STUDY DIVERSION?
Post-arrest diversion programs are often offered as alternatives to incarceration for persons who have been arrested for various charges including drug possession and prostitution. Diversion programs have different requirements for success, but nearly all include avoiding any illicit behavior or behaviors theorized to lead to illegal acts. One of the better known diversion programs is called Drug Court, which is implemented under the auspices of judicial correctional departments and includes offerings such as drug treatment, medication-assisted treatment [MAT], and case management. The markers of success include stabilization in housing, successful drug abstinence or compliance to an MAT regimen (confirmed via regular drug testing), and adherence and punctuality to regular meetings with case workers. Another important diversion program is for persons arrested for sex work.
PROJECT DAWN COURT: Philadelphia’s Prostitution Diversion Program
The diversion program in Philadelphia, Project Dawns Court defines all sex work as violence against women and is not open to trans women or cisgender men. Established in 2010, it assumes that most members enter sex work to re-enact trauma. The program mandates that sex workers abstain from doing sex work and using illicit substances, andrequires members to engage in trauma counseling. The District Attorney’s Office recommends cisgender women who have at least three prostitution charges to the program and no violent charges on their record.
Once admitted, defendants undergo a Forensic Intensive Recovery (FIR) evaluation and must complete four phases: 1) abstain from substance use for 30 days; 2) attend 90 days of out-patient services; 3) undergo 120 days of intensive treatment for sexual trauma; and 4) participate in 120 days of reintegration preparation which could include services such as parenting classes. Members must appear in court at least once a month (or more if deemed necessary by the judge and prosecutors) for assessment. If a participant is unable to complete the requirements or tests positive for drugs, she has to restart the phase and do “sanctions” such as writing an essay or doing community service. After graduation, members must avoid drug and prostitution charges for a year before the precipitating charge is expunged. The rest of their records remain intact.
Project Dawn Court is problematic for sex workers for several reasons. The program is not automatically open to anyone with repeat prostitution charges; members are handpicked by the DAO. Courts take on a paternalistic role and infantilize women by becoming involved in every aspect of their lives. For instance, if a participant takes on a new job or moves into a new home, this decision is scrutinized intensely by court staff. The boundaries between the therapy room and the courtroom are non-existent and this is intentional. Mary DeFusco, co-founder of the program, said “The judge becomes a part of the person’s therapy. The [women are] always thinking in the back of their mind, ‘what would the judge say?’” CITATION
Project Dawn Court mandates therapy for sex workers and requires that therapists be willing to share what occurs in session with the court. This is ethically problematic and creates a lack of safety and trust for those in the program by linking therapy to punishment and surveillance. In many ways, these programs can in fact recreate the dynamics of abuse that survivors of gender-based violence experience by forcing them to undergo constant monitoring (Sweet 2021). It is unethical to coerce someone into healing with the threat of incarceration.
The program also does not adequately prepare members for a career change. An evaluator for the program found that several graduates ended up working low wage jobs that were hard to get to and did not offer enough hours for a living wage. Others could not access jobs because they could not pass the criminal background check. In many ways, the court is a set up: members have no choice to but to return to sex work to make ends meet, which not only prevents them from getting their records expunged if they are prosecuted again, but also will result in incarceration. This system of “alternatives” does not offer any support structure or basis for transition but only exists as a wall that sabotages individuals for increased chance of incarceration.
HOW WAS THIS RESEARCH DONE?
Project SAFE members, who had lived experience of sex work, drug use and homelessness, created a survey to understand how sex workers and people who use drugs navigate the multiple systems in their lives– criminal justice, medical and mental health– to access services and reduce harms.
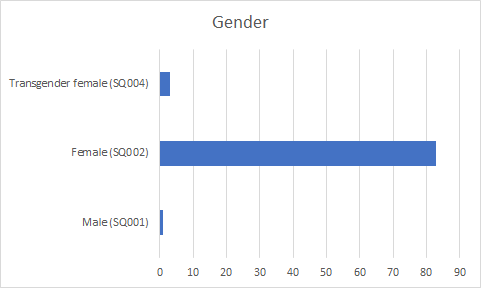
We developed and conducted the survey in 2017. We initially surveyed five community members who received services at either our community space or via the deliveries network to gauge the effectiveness of the questions. We also solicited feedback on language used in the survey after and then revised it. We trained an additional three community members to do data collection along with the five members who produced the survey. We then surveyed an additional 89 people. Inclusion criteria was women, queer and gender nonconforming indivudals who utilize Project SAFE services and are 18 years or older.
We recruited members by doing outreach in the Kensington neighborhood and asking survey members to refer community members. We collected data at the Project SAFE community space and gave members $20 in cash for their time through a grant from the Criminal Justice Initiative. We entered and analyzed data via LimeSurvey. We collected a total of 89 surveys. While we entered every survey into our statistical reporting program, we note that most surveys were incomplete. We asked community members to only fill out what they were able. Our particpants were dealing with unmanaged pain and withdrawal, exhaustion, and/or preoccupation with immediate unmet needs, which sometimes made them unable to complete the full survey. As a result, we report completed numbers and missing data by question instead of overall.
It is important to note that between when we conducted the survey and when we were able to analyze and write the findings, the COVID-19 pandemic deeply affected our members. This world-shaping event affects our findings… As such, we include personal narratives from our community members in order to provide more in-depth context to the findings that we report here, but these were not part of the survey.
FINDINGS AND RECOMMENDATIONS
EXCLUSION FROM SOCIAL AND LEGAL SERVICES
Although the Kensington neighborhood and the city of Philadelphia are peppered with social service providers, our members reported that their basic material needs are largely unmet due to both structural barriers and circumstances created by the everyday difficulty of surviving poverty. Many of the respondents also discussed how criminalization of survival strategies such as selling drugs and trading sex also negatively impact their ability to access services.
Sex work is a common experience among our members at Project Safe. In line with this, most of our members in the survey said that they traded sex for housing, drugs, or food. 60 members (71.4%) answered yes, out of 84 completed questions. Another 13 members reported having traded sex in the past. Of these members, 42 or 65.6% reported having other means of income besides sex work, out of 58 completed answers. Other sources of income included informal money like support from a husband or boyfriend, selling drugs, babysitting or cleaning houses, or panhandling, as well as formal money from Social Security or Public Assistance.
Drug use is also very common among our members at Project Safe and in the unhoused communities in Kensington and Hunting Park. Our survey results confirm this as well. Of 85 complete answers, 82 members or 96.5% reported using drugs. members self-reported how often they use drugs in an open-ended question, meaning they could describe their usage frequently however fit their experiences best. 78 members answered this question. Nearly all used drugs everyday or most days. 82 members explained what drugs they used, with marijuana, K2, powder cocaine, rock cocaine, fentanyl, and heroin being frequent answers. 80 members explained which drugs were their favorites. Many liked heroin the most, with others liking marijuana, fentanyl, and alcohol the most.
Many members had ongoing health problems and disabilities. Out of 82 people who answered the question, 64 or 78% reported having a current health problem or concern. members shared a variety of problems and concerns with us, from chronic preventable illnesses such as Hepatitis C, emphysema and COPD, and high blood pressure or heart disease. Others had chronic pain conditions, ranging from arthritis to back pain. Several members shared that their chronic pain had been made worse by having to delay treatment. Still others had dental problems, untreated abscesses, and reproductive disorders like prolapse. 34.4% (21) reported having been diagnosed with a behavioral or learning disability, while 16.2% (12) had a physical disability. In addition to physical illness and pain, many of our members experienced mental health concerns. 61 members, or 72.6%, had a current mental health concern. 75.6% (61) of our members had been to a mental health provider. Of these, 91.9% (57) had received a diagnosis. Our members shared with us a number of common (and stigmatizing) diagnoses, such as bipolar disorder, schizophrenia, ADHD, depression, and anxiety, while many shared diagnoses and experiences of PTSD with us.
What are the most needed services? (i.e. 1 in 2; more than half)
In order, the most needed services were: housing (85.9%), transportation (82.4%), meals (65.9%), laundry and shower (63.5%), substance use treatment (61.2%), mental health treatment (60%), and healthcare (56.5%). Several members also shared with us a need for employment or job training.
Likewise, our members had unmet needs for legal services. In order, the most needed services were: benefits like Medicaid and SNAP (47.1%), help with outstanding warrants (31.8%), custody of children (25.9%), housing or eviction assistance (23.5%), access to financial services (11.8%), protection from abuse (5.9%), and immigration (3.5%). members also shared needing access to agencies that can provide basic legal documents and identification cards.
A misperception that often occurs when planning services is that they should focus on younger demographics. Our research shows that community members range in age from age 19 to 58 with an average age of 38 and so services should collectively address this spectrum.
Barriers to Accessing Existing Services
Our members reported many barriers to accessing existing services. Lack of transportation was a common barrier (52.9%), while confusion about how to access services was another (44.7%). Other members reported barriers like lack of identification (40%) and lack of time (34%) or work schedule (17.7%). Disability, discrimination, and fear of reprisal played a role as well, with members reporting barriers like medical conditions (25.9%), active warrants (23.5%), discrimination or bias (24.7%), and citizenship status (2.4%).
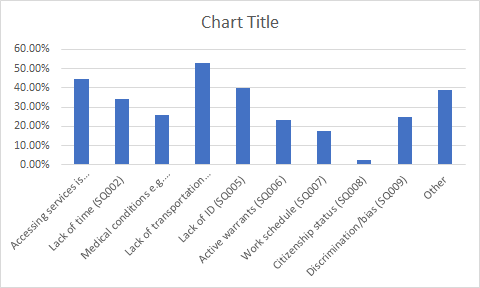
Our members shared other barriers with us in open-ended comments. Several members shared that their substance use itself posed a barrier; being dopesick or feeling run down from hustling made it difficult for them to seek services. A few members also shared with us that forms of exhaustion with simply struggling to survive made it difficult for them, saying things like: “feel I don’t deserve,” “feeling inadequate, not good enough,” and “round around and nonresponsive.” Being on the run for drugs or sex work, or from active warrants, also made our members too tired to try accessing services. Two even said simply: “I don’t know where to start.”
Recommendation 1: the City of Philadelphia should divert funds earmarked for policing and prosecution of people who trade sex and use drugs to service providers committed to providing principled harm reduction services and legal services.
Recommendation 2: Provide no-barrier* high quality services that are either located near transportation hubs or that provide transportation to people using services.
Recommendation 3: Hire people who use drugs and trade sex to work as community navigators who can assist their community members in connecting to services. These community navigator positions would adhere to workers rights standards, and provide ongoing training opportunities so that community members could advance in their careers in the sector.
*No-barrier services do not turn away potential clients due to lack of identification, money, criminal history, disability, etc. They provide service to the best of their ability to every individual who contacts them for services.
EXPERIENCES OF DISCRIMINATION: NOT WELCOME ANYWHERE
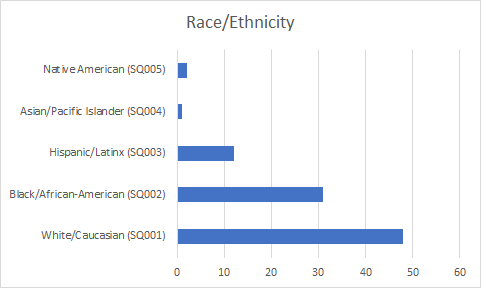
Our members reported experiencing stigma and discrimination in a range of public spaces and facilities due to being perceived as people who use drugs, trade sex and/or are unhoused. Race and gender identity compounded the stigma. About half of all respondents were people of color (one third identified as Black or African American, ten percent identified as Hispanic or Latinx, one as Asian or Pacific Islander, and two as Native American).
Overall, mistreatment based on these oppressed identities eroded trust with healthcare providers, prevented our members from seeking the help and care that they needed and led to poor health outcomes including chronic illness, life-threatening infections and premature death.
Where are people who use drugs and trade sex most likely to experience mistreatment and/or forced removal?
We asked members where they had been kicked out of or had experienced mistreatment. One third of our members said they experienced these problems at jobs. A similarly high level of mistreatment occured in housing. Public places like bars, restaurants, and stores were also common sites of mistreatment for our members. Our members were also mistreated in social service agencies such as government offices, healthcare facilities, and schools . Almost 40% of our members who answered the question said that they believed this mistreatment was because they were perceived as trading sex, while nearly 80% believed this mistreatment was because they were perceived as using drugs. Members listed other reasons, with racism and sexism being very common open-ended answers. For example, one person who had been kicked out of school shared with us: “I told the principal I’d kick her ass because she called me a spic.”
The link between mistreatment in healthcare facilities and poor health outcomes
Our members reported experiencing stigma and discrimination frequently when seeking healthcare, which had profoundly negative effects on their well-being. Of those who answered the question, about half had been searched in a medical or hospital setting or been discriminated against or mistreated, and about one third had been denied access. Most of these experiences of stigma and bias occurred in the Emergency Department (60%), but they also occurred in inpatient hospital clinics and outpatient hospital clinics, as well as other spaces such as the dentist. One participant shared with us an example: in a mental health facility, she was blamed as a teenager for supposedly “leading on” the uncle who raped her. While about half (44%) of our members believed this was due to the perception that they traded sex, a large majority (88%)believed it was due to the perception that they used drugs. Members also shared with us that being unhoused had led to their poor treatment. Several said things like “smelling bad,” “homelessness,” “not having showered,” and “Black and poor” as reasons for their mistreatment. Both trans women who completed the survey shared that they had experienced transphobia while seeking healthcare.
Mistreatment led to or included poor healthcare for our members. The majority (57%) had their pain under-or inadequately treated. The majority (54%) also had their symptoms or medical complaints ignored. About half (48%) had their non-pain related complaints ignored. One participant shared what mistreatment was like: “Disrespected, made to feel like shit, scared of being reported to the police.” This type of mistreatment causes our members to delay or avoid care, and to lose trust in healthcare providers. This aligns with our findings above about health problems — many members reported chronic injuries and illnesses due to lack of treatment. As these findings demonstrate, stigma and discrimination among healthcare providers drives unhoused people who use drugs or trade sex away from essential healthcare.
Disclosing drug use and sex work status to healthcare providers
Our members make decisions about how they interact with healthcare providers based on prior experiences. Of those who answered the question, only 43% said they’d disclosed to medical providers that they trade sex. members shared their reasons why not, ranging from things like “Felt weird,” “embarrassing,” and “fear,” to “They would think poorly of me,” “bad enough w/o that,” and “Not their business.” Of those who disclosed, though, about half (44%) said they were treated well and about one third (34%) said they were treated badly. The rest said it depends or didn’t change their treatment. Just 15% of those who answered the question said that this disclosure improved their quality of care, while over half (54%) said it did not change the quality of care, and one third (31%) said it harmed the quality of care. As a result, the majority of our members (66%) did not trust medical providers to provide good quality care to people who trade sex.
Our members had similar, but somewhat better, experiences around disclosure of their drug use. Most of our members who answered the question (83%) had disclosed that they used drugs to a medical provider. Reasons for not doing so were similar to the question above about trading sex: “Fear of dscrimination,” “afraid of judgment,” and “ashamed.” However, trading sex may be stigmatizing but more easy to hide or allowing our members more agency around disclosure. Involuntary drug testing in inpatient and outpatient clinics takes away this ability to choose based on how safe a participant feels: one told us “no [she did not disclose,] but I had dirty urine.” about half (46%) of our members who answered the question said that they were treated well as a result, and one third (32%) said that they were treated poorly. Another one fifth (22%) said it depends. Members were much more likely to say that disclosure harmed or did not change their quality of care. Of those who answered the question, less than one tenth (9%) said it improved the quality of care, half (51%) said it did not change the quality of care, and less than half (4!%) said it harmed the quality of care. These experiences shaped how trustworthy our members viewed healthcare providers in terms of providing good quality care to people who use drugs. While the level of trust is slightly higher than around sex work, over one third (3*% of our members do not trust providers.
Healthcare facilities are sites of medical trauma
As we noted above, these experiences of stigma and discrimination drive our members away from healthcare. Of those who answered the question, most (62%) had discharged themselves Against Medical Advice (AMA) due to mistreatment and discrimination. Similarly, over two thirds (70%) of members who answered the question had avoided healthcare due to unwillingness to interact with providers. The majority of members (68%) said they’d avoided care because of dislike or fear of providers, while other almost half (43%) said they did so because of negative stories from others, and another third (30%) said they did so because of inaccessibility or lack of transportation. Our members shared other reasons with us, too, such as embarrassment and shame, lack of health insurance, and fear about the outcome. Other members shared that they learned how they would be treated from observing others: “Fear of stigma/judgment from persons in the waiting rooms” and “Witnessing healthcare providers ‘treating others like shit.’” Some shared that they hate hospitals due to traumatic experiences in them. One participant shared: “Didn’t want to hear bullshit from doctors who think everything has to do with drugs.” This aligns with members’ fear and personal experiences that their pain would be dismissed or poorly managed, and their symptoms or complaints would be dismissed.
Overall, our findings in this section align what we already know from the literature on the harmful effects of stigma and discrimination on health outcomes and on the provider-patient relationship. Our members avoided care for ongoing health problems because they had been treated badly. Providers frequently hold problematic and stigmatizing assumptions about marginalized groups–especially Black and Brown people–and these biases lead them to provide worse quality care (Manzer and Bell 2021). Mistreatment drives people who are already vulnerable away from seeking care and increases existing inequalities in health and life expectancy (Manzer and Bell 2021; Williams 1999). Experiencing discrimination in general makes people’s mental and physical health worse (Thoits 1995; Williams 1999). Our participants’ experiences are similar to those that sex workers have documented worldwide in soceities where sex work is criminalized and stigmatized. For example, in a sex worker-led study in four countries in southern Africa, sex workers were treated badly, denied care, and unable to access STI treatment and condoms (Scorgie et al). However, this study confirmed that clinics created to serve sex workers provided much higher quality of care and addressed unmet healthcare needs among sex workers. We join the authors of this study in calling for more clinics designed to serve sex workers and more sensitivty trainings for providers. Many of our members said that their treatment depends on the provider. This indicates that providers can also exercise agency in treating people who they perceive or know to be unhoused, trading sex, and/or using drugs by providing humane, compassionate, and competent care that takes into consideration structural and material constraints on people’s lives.
Recommendation 1: Mandate harm reduction training for all medical and mental healthcare facilities that receive public funding. These trainings should center the voices and experiences of people who use drugs and trade sex. Include PWUDs and sex workers as paid participants in the design and implementation of these trainings.
Recommendation 2: Establish a “Bad Encounter Hotline” to enable PWUDs and sex workers to report experiences of discrimination and institutional violence. The hotline should be fully funded via public funds and accountable to a regulatory board comprised of PWUDs and sex workers.
Recommendation 3: Compile and publicize a list of mental and medical healthcare providers who provide compassionate and trauma-informed care to PWUDs and sex workers. The list should be updated annually and service providers would need to get certified to be included as detailed in Recommendation 1.
Recommendation 4: Establish clinics and community-led public health interventions staffed and run by sex workers and PWUDs using existing models such as St, James Infirmary and Ashodaya Samithi (an organization run by and for sex workers of all genders in Mysore, India).
ENCOUNTERS WITH VIOLENT SYSTEMS AND INSTITUTIONS: LAW ENFORCEMENT, PRISONS AND COURTS
Experiences with policing are pervasive for our members and produce a range of harms including trauma incurred through the process of arrest, detention and incarceration; disruption of services such as MAT; loss of housing and custody of children, etc. Prostitution and drug-related charges also make it difficult, if not impossible, for our members seeking to secure jobs outside of the sex and drug industries. Sex work and substance use are intertwined activities for most of our members who report using a significant portion of income raised from trading sex towards the purchase of substances. The amount of time spent raising the money to purchase a day’s supply often occupies the majority of our members’ time. For this reason, we propose that the City of Philadelphia work towards establishing safe supply programs, which provide pharmaceutical grade opioids and stimulants to people at risk of overdose or other medical complications from using an adulterated drug supply. Medical providers distribute the drug to clients and monitor their use. Positive outcomes include decrease in overdoses, stabilization of drug use, and an increased ability to use sex work income for other needs.
Experiences of arrest
This experience is expressed in our survey as a large number of arrests and lengthy tenures of incarceration, and with a failure in diversion programs to be offered or useful to members. We asked our members how many times they’d been stopped by police. Of the 66 who answered, the average number of stops was 87. The fewest number of stops was zero and the highest 1000, and half of our members had been stopped between 5 and 26 times. Of those who answered, 89.9% (71) had been arrested. The average number of times our members had been arrested was 10, with the fewest being 1 and the most being 100. Half of our members had been arrested between 2 and 15 times.
What are the most common charges?
We asked our members to select what they’d been charged with from a non-exclusive (i.e., they could select any and all that applied) list. Unsurprisingly, the two most common charges were drug-related (75.3%) and prostitution-related (49.3%). The next two most common were shoplifting (32.9%) and violation of probation (27.4%). Our members were also charged with assault or other violent offenses (19.2%) and burglary (11%). Finally, our members also had been charged with a range of charges related to being unhoused, like trespassing (10%), loitering (5.5%), disorderly conduct (12.3%), and resisting arrest (12.3%). Our members also faced other charges (19.2%), such as DUI, falsifying ID, and criminal mischief.
Experiences of incarceration
Such a high number of encounters with police led to many experiences with incarceration as well. Of those who answered, 95.8% (69) had been locked up an average of 9 times. Half our members had been locked up between 2 and 9.5 times, with the least number of times being 1 and the most being 100. The shortest time our members had been locked up in one stint was 3 days and the longest was 3 years. The shortest total amount of time our members had been locked up was 5 days and the longest 15 years. Of those who answered, 14.7% (10) had spent time in prison, although no one was currently on state parole. 35.8% (24) of those who answered were currently on county probation and 38.2% (26) had an active warrant out. On average, members had 2.3 active warrants out, with half having between 1 and 3, with the most common charges being violation of probation and drug-related charges, although some members told us they had failure to appear warrants and traffic citations. These findings align with what we reported above regarding barriers our members face in seeking social services: active warrants prevent them from accessing housing, material support, and getting IDs.
Relationships with law enforcement
These experiences with arrest and incarceration affected how safe our members felt reporting crimes that had happened to them. Members tended to feel safe filing reports, but did not trust police officers to do anything about those reports. 65.3% (47) of those who answered felt comfortable reporting stalking, rape, or assault to the police, while 60.8% (45) felt comfortable reporting robbery. However, less than half (47.1% or 33) thought that the police would take a report filed by them seriously. 63.6% (42) had had a bad experience with the police. On the other hand, 90.6% (58) said they would report a bad date to Project SAFE if they experienced violence while trading sex.
Experiences with diversion programs
Our members had experiences with diversion which they found did not meet their needs. Only 46.5% (33) of those who answered had been offered a diversion program. The three most common programs were accelerated misdemeanor programs, Project Dawn Court, and Drug Treatment Court, for drug-related and prostitution-related charges. 5 of our members said that they’d participated in Project Dawn Court. 59.5% (25) of members said they would have participated if offered. The main reason our members did Project Dawn Court was avoiding jailtime, though accessing drug treatment was another frequent answer. For those that weren’t offered Project Dawn Court, avoiding jailtime was again the main motivator that would have made them participate. If members declined or would have declined, their main reasons for doing so were that the program had too many requirements, it felt like they were being set up to fail, and it merely delays (but does not avoid) incarceration. Of our 5 members who had been through Project Dawn Court, 4 completed it. All 4 said that drug treatment was helpful and 3 said that counseling was helpful. However, just 3 of the 5 said they’d recommend the program to others. Housing, transportation, and job training were needs that were not met by the program.
Recommendation 1: Decriminalize sex work.
Recommendation 2 : Decriminalize drug possession, use and selling.
Recommendation 3: Redirect vice unit budgets towards safe supply programs. A description of safe supply and the evidence-base for them is included in the What Works section.
Recommendation 4: Redirect vice unit budgets towards harm reduction based social services including housing, medical and mental healthcare and transportation.
Recommendation 5: Establish a Citizens Oversight Board that has positions reserved for PWUDs and sex workers.
OVERDOSE EPIDEMIC
Overdose Overview
Since the start of the global coronavirus-19 emergency, the already dire fatal opioid overdose crisis has worsened in North America.1 In 2019, 49,850 individuals sadly lost their lives, which accounts for over 70% of all overdose deaths (CDC, 2021). Overdose risk is amplified by injection, which is a mode of drug administration associated with a host of adverse health outcomes including HIV, Hepatitis C, and other serious opportunistic infections leading to abscesses, infective endocarditis, spinal osteomyelitis, sepsis, and possibly death.2,3,4 In addition to these health issues, drug-related harms are also characterized by participation in “illicit” behaviours to procure drugs.5 Finally, the adulteration of the unregulated opioid supply with fentanyl, a far more potent and shorter-acting opioid than heroin, has increased overdose risk and number of daily injections, subsequently increasing risk of all aforementioned health and social issues.6
Experiences of Overdose
A little over half (55.1% or 43 people) of our members who answered the question had overdosed on drugs. On average, members had overdosed about five times (mean=4.9), with half having overdosed between 2 and 5 times. Most commonly, members overdosed on heroin and fentanyl. An overwhelming majority of members (92.1% or 70 people) said they’d witnessed an overdose. On average, our members had witnessed about 35 (mean=35.2) overdoses, with half having witnessed between 2 and 35. These results confirm that overdose is a common and life-threatening experience among unhoused people.
Community Response to the Overdose Epidemic
However, in line with previous findings [?] and with our commitments as Project Safe, our survey also demonstrates that community care is essential. 70.4% (51) of members had administered Narcan, on average 26 times. Half of our members had administered Narcan between 2 and 23.75 times. 95.3% (61) of our members would call 911 if they witnessed an overdose. However, only 19.4% (13) said they tested their drugs for fentanyl. The responses our members gave us about these findings are helpful for putting them in context. One participant shared with us that they would call 911 if they had access to phones, making cell phone access for unhoused people a life-saving priority. Several other members shared with us that they distribute Narcan to their community members, including the people they buy drugs from, in order to prevent overdose deaths. [Public phones]
RESOURCES
B Chapman-Schmidt, ‘“Sex Trafficking” as Epistemic Violence’, Anti-Trafficking Review, issue 12, 2019, pp. 172-187, www.antitraffickingreview.org
Deering KN, Amin A, Shoveller J, Nesbitt A, Garcia-Moreno C, Duff P, Argento E, Shannon K. A systematic review of the correlates of violence against sex workers. American Journal of Public Health. 2014;104:e42–e54.
Reza-Paul, S., Steen, R., Maiya, R. R., Lorway, R. R., Wi, T. E., Wheeler, T., & Dallabetta, G. (January 01, 2019). Sex Worker Community-led Interventions Interrupt Sexually Transmitted Infection/Human Immunodeficiency Virus Transmission and Improve Human Immunodeficiency Virus Cascade Outcomes: A Program Review from South India. Sexually Transmitted Diseases, 46, 8, 556-562.
Paige L. Sweet. 2021. The Politics of Surviving. University of California Press.
Vanwesenbeeck, I., & SpringerLink (Online service). (2017). Sex Work Criminalization Is Barking Up the Wrong Tree. (Archives of sexual behavior.)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5529480/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3359131/
https://www.ohtn.on.ca/wp-content/uploads/2020/04/RR_safe-supply.pdf
The effectiveness of compulsory drug treatment: A systematic review
https://www.sciencedirect.com/science/article/abs/pii/S0955395915003588
Hoots and harm reduction: a qualitative study identifying gaps in overdose prevention among women who smoke drugs
https://harmreductionjournal.biomedcentral.com/articles/10.1186/s12954-021-00479-3
Ethical and HumanRights Issues in Coercive Interventions with Sex Workers, Affilia: Journal of Women and SocialWork 28(4) 344-349 The Author(s) 2013 Reprints and permission:sagepub.com/journals Permissions.nav DOI: 10.1177/0886109913505043aff.sagepub.com http://www.bestpracticespolicy.org/wp-content/uploads/2013/10/Affilia-2013-Wahab-344-9.pdf
1. Toronto Public Health reports record number of overdose deaths. January 29, 2021. https://www.toronto.ca/news/toronto-public-health-reports-record-number-of-overdose-deaths/. Published 2021. Accessed January 29, 2021.
2. Kerr T, Wood E, Grafstein E, et al. High rates of primary care and emergency department use among injection drug users in Vancouver. J Public Health (Bangkok). 2005;27(1):62-66. doi:10.1093/pubmed/fdh189
3. Takahashi TA, Baernstein A, Binswanger I, Bradley K, Merrill JO. Predictors of Hospitalization for Injection Drug Users Seeking Care for Soft Tissue Infections. J Gen Intern Med. 2007;22(3):382-388. doi:10.1007/s11606-006-0079-y
4. Werb D, Garfein R, Kerr T, et al. A socio-structural approach to preventing injection drug use initiation: rationale for the PRIMER study. Harm Reduct J. 2016;13(1):25. doi:10.1186/s12954-016-0114-1
5. Lovell AM. Risking risk: The influence of types of capital and social networks on the injection practices of drug users. Soc Sci Med. 2002;55(5):803-821. doi:10.1016/S0277-9536(01)00204-0
6. Ciccarone D. Fentanyl in the US heroin supply: A rapidly changing risk environment. Int J Drug Policy. 2017;46:107-111. doi:10.1016/j.drugpo.2017.06.010
7. National Institute on Drug Abuse. Medications to Treat Opioid Use Disorder. Natl Inst Drug Abus. 2018;(June):1-47. https://www.drugabuse.gov.
8. Maghsoudi N, Bowles J, Werb D. Expanding access to diacetylmorphine and hydromorphone for people who use opioids in Canada. Can J Public Heal. 2020;111(4):606-609. doi:10.17269/s41997-020-00315-4
9. Rai N, Sereda A, Hales J, Kolla G. Urgent call on clinicians: prescribe alternatives to poisoned drug supply. Heal Debate. 2019.
10. Government of Canada. No Title. https://www.canada.ca/en/health-canada/news/2020/09/government-of-canada-highlights-support-for-safer-drug-supply-projects-in-ontario.html. Published 2020. Accessed March 22, 2021.